
This article has been peer-reviewed under the direction of Professors Mary Elizabeth Leighton and Lisa Surridge (University of Victoria). It forms part of the Great Expectations Pregnancy Project, funded by the Social Sciences and Humanities Research Council of Canada. [Click on the image to enlarge it.]
Miscarriage in Nineteenth-Century America
In 1867, a Mrs. M. of Ursa, Illinois called upon physician John C. Pearson after she miscarried in the fourth month of her pregnancy. Mrs. M delivered the fetus easily on her own but continued to bleed heavily as the placenta remained behind. Pearson attempted to help her deliver the placenta with “gentle means” such as “irritation of the os [the opening of the cervix] with the finger for a few minutes.” Seeing no progress, Pearson then proceeded to pack the vagina with cloth, a process that physicians of the time referred to as “tamponing” and then left the woman, promising to return the next day. Upon his return Pearson was gratified to see the placenta “lying loose in the vagina,” from where he could remove it without any trouble or pain to his patient. In his report of this case in the Medical and Surgical Reporter, Pearson championed the tampon as the best treatment for retained placenta, as it avoided “the great pain of introducing the hand up to the fundus of the uterus and by violence tearing away the after-births.” Keeping the comfort and safety of his patient in mind, Pearson repeatedly condemned the use of metal instruments for encouraging a miscarriage to completion.
A bourgeois wife shows her husband the preserved fetus of her cousin. [S.G.C. Garvani]. Courtesy of the Wellcome Collection.
The primary medical concern about miscarriage in nineteenth-century America was the possibility of retained placenta or fetal tissues. In the wake of a pregnancy loss, if any fetal or placental tissues remain in the uterus, the woman will continue to bleed and face the possibility of fatal hemorrhage or infection. Medical journals between 1830 and 1870 were full of accounts of doctors visiting women who bled for days or even months after a miscarriage. But, in most of these accounts, physicians relied upon tamponing or the use of ergot (a natural fungus known for centuries to induce uterine contractions), gentle methods that required little in the way of intrusion into the uterus.
By the end of the 1800s, physicians’ writings about miscarriage were completely different. In the last two decades of the nineteenth century, American doctors seemed agreed that the best course of action in all cases of miscarriage was immediate and instrumentally intrusive action to clear the uterus. The tampon was no longer the treatment of choice; instead, doctors opted for metal instruments to scrape out the uterus and prevent complications. Why this reversal? Why had Pearson’s gentle methods fallen out of favour? Well, it turns out that a lot had changed in American society between the 1850s and the 1880s, and these changes, while not directly related to medicine, had a lasting impact on physicians’ approach to miscarriage.
Terminology
In nineteenth-century America (and throughout much of the twentieth century), the words “abortion” and “miscarriage” were interchangeable. Women wrote of an “abortion” in a way that clearly indicates that the event was neither intended nor induced, while doctors described “abortions” with a variety of causes, most being accidental. The medical crusade against the practice of intentional abortion in the 1860s led doctors to use the phrase “criminal abortion” more often, but this adoption was not widespread or reliable. Even today, many clinical descriptions of miscarriage use the word “abortion.”
Industrialization and Medicalization
Starting in the 1850s, the United States experienced rapid industrialization and saw unprecedented immigration, altering the logistics and meaning of family and reproduction. As manufacturing increased with the Industrial Revolution, male and female workers moved into cities, leaving many of their traditions behind along with their extended families. These newly urban workers, separated from families and familiar communities, lost access to traditional and folk knowledge of health, illness, and miscarriage. Some workers found themselves an ocean away from familiar reproductive knowledge and practices as immigration rates, which had measured around 60,000 a year in 1800, sharply rose to almost 2 million a year by 1850.
In 1850, white male physicians delivered around 10–20% of American babies and attended even fewer pregnant and miscarrying women. Most of the families who did rely on doctors for childbirth at this time were wealthy and educated, viewing medical aid as evidence of their high positions in society. But as urban working populations grew and American doctors became interested in gaining clinical experience during their training, white upper-class male physicians began attending in childbirth to more and more poor women, immigrants, and women of colour in ways they never had before.
Starting in the 1870s and 1880s in large cities like Boston and New York, but also in smaller manufacturing towns along the east coast, immigrant groups sought out physicians in much larger numbers. Women who could not afford a physician or midwife, did not have the space to give birth in their homes, were separated from the assistance of family, or who could not admit their pregnancies to their family (usually because they were unmarried) needed a new location to give birth. Charitable hospitals and dispensaries fit that bill, with some already in existence, and many more being built at this time for this very purpose. These locations also became useful to women experiencing miscarriage who could not get help elsewhere. However, increased interactions between educated white physicians and disempowered women over miscarriage were not a trends limited to large urban centres or charitable hospitals.
Miscarriage and Race
Many families who resided outside large cities but were still employed by the broader industrialized world looked to physicians for aid in cases of miscarriage, such as the patients of Charles Brayton. Brayton was one of nine physicians in the town of Stonington, Connecticut, a seaside community that served as home to many immigrants who worked in the wool and cotton mills, in the vibrant shipping industry, or as servants in the houses of the more prestigious white families in power. In 1880, Stonington was home to just over 7,000, 17% of whom were foreign born, 38% of whom had at least one foreign-born parent, and 3% of whom identified on the census as “black” or “mulatto.” By comparison, of the women who sought out Dr. Brayton in cases of miscarriage, 47% were immigrants and 8% were identified by Brayton as “colored”.
While working-class immigrants comprised a minority of Stonington’s overall population, they ended up accounting for the majority of Brayton’s patient base in cases of miscarriage. Couples such as Louis and Louise Rassum from Germany, Joseph and Delphina Maraya from the Azores, Olaf and Josephine Rood from Norway, and Michael and Catherine Harrington from Ireland all sought out Brayton for aid, most likely because they had left family and traditional healers behind in their home countries. As American doctors began seeing more and more miscarriage cases, they began to change how they understood their own role in the event and sought to increase their business and authority over the medical meanings of miscarriage. We should not forget that they succeeded in the medicalization of miscarriage not because they had better treatments of preventative methods than any other medical or lay person, but rather because women like Delphina Maraya had nowhere else to turn when she began bleeding in the fourth month of pregnancy.
And, unlike in previous encounters with moneyed white women, as doctors began interacting with poor, immigrant, and Black women they saw opportunities to use these miscarriage cases as learning and experimental experiences. By the 1840s white male physicians had been building a stable foundation for their role in the birthing process based upon social and scientific understandings of race and ethnicity. To argue that they were the better attendants for birthing women, doctors perpetuated a narrative of racial and ethnic difference in reproduction. They claimed (as George Engelmann did in 1883) that groups that were “closer to nature” or “more animalistic” (typically African Americans, Native Americans, and eastern European immigrants) did not need medical help in childbirth because they were naturally better at the job. But white, “civilized” women were removed from ancient natural knowledge and couldn’t possibly take care of matters on their own.
Physicians seized upon these narratives as a rationale behind their authority in the bedrooms of white middle- and upper-class women, but doctors were not the only ones who saw benefit in this biological construction. White enslavers supported, perpetuated, and benefitted from the construction of white female bodies as “civilized” and susceptible to damage through pregnancy and birth, while Black female bodies were perceived as “primitive” and better equipped to give birth easily, without pain, and numerous times in their lives. These biological notions of race and reproduction helped support the most profitable mechanism for many white Americans: slavery.
If physicians and enslavers believed that Black women were naturally impervious to pain and lacking in the gentler emotions of white women such as maternal love and sexual modesty, then some of the more horrific practices under slavery including rape, separation of women from their infants, or demanding women go back to grueling work hours after giving birth could be scientifically supported.
These narratives survived emancipation and were firmly entrenched in American medicine and white society at large by the 1870s, as more white physicians found themselves involved in miscarriage cases with poor women, immigrants, and women of colour. The view of the hardened bodies of “primitive” women that doctors encountered in miscarriage cases allowed them to intrude upon these bodies in ways that would not have been appropriate or even allowed if the bodies had been white and upper class.
If a physician believed that the miscarrying woman at a charity hospital or dispensary was less delicate, in physical health and in sensibilities, than his white private practice patients, he might not have thought twice about sticking one or both of his hands up into her vagina and uterus and jabbing a sharp metal instrument into her birth canals. In fact, this mindset had already cemented many American doctors’ international esteem in the field of gynecology. It was in this setting that American physicians experimented with and subsequently developed a routine miscarriage treatment: “to empty the uterus as soon as that can be done with safety, to thoroughly ascertain that it is entirely emptied and never cease supervision of the case until that end is accomplished,” (Martin).
To be sure, in some cases of miscarriage, emptying the uterus (what we would now call dilation and curettage, or a D&C) was necessary. If any fetal or placental tissue remained inside a woman's uterus, she could face extensive bleeding, infection, and even death. However, prior to the 1860s, physicians and women agreed that such invasive action was only necessary in the minority of cases that did not quickly resolve themselves. Many women experienced miscarriage without any such threat, but, as the century progressed, physicians attempted to convince potential patients that every miscarriage should be treated as a dangerous event.
By the 1880s, many teaching texts and medical journals recommended emptying the uterus with metal instruments like curettes, often using words like “scraping,” “force,” and “violence,” (Shivers, Garrigues). This intrusion into women’s bodies in a newly intimate and often violent matter was only made possible by the poor women, immigrants, and women of colour who, out of desperation, called for help when they found themselves bleeding and in pain.
Perceptions of Miscarriage
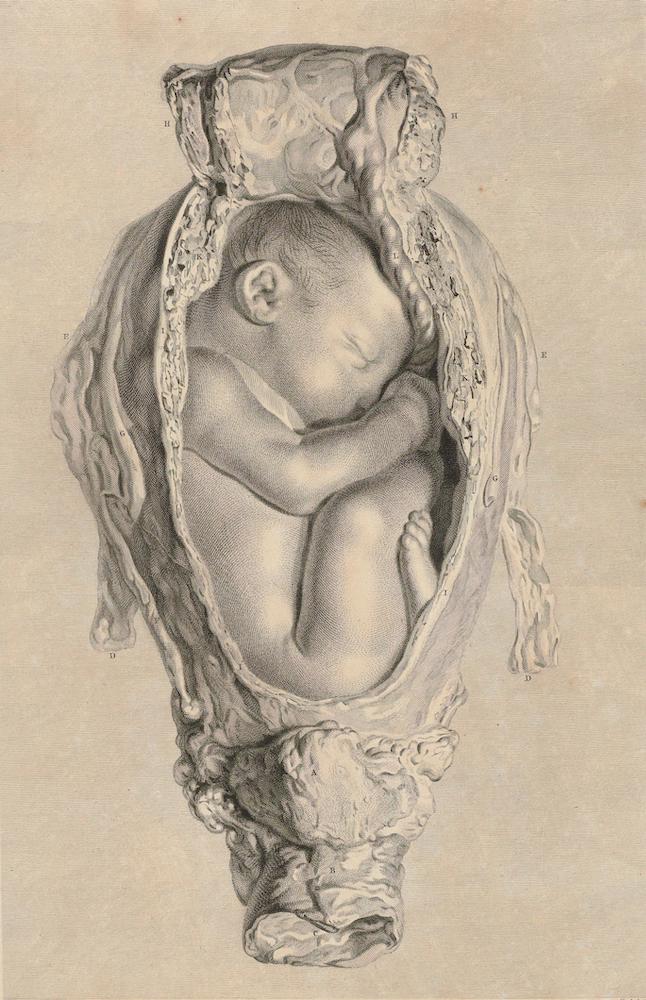
Anatomia uteri humani gravidi tabulis illustrata ... The anatomy of the human gravid uteris exhibited in figures [William Hunter]. Courtesy of the Wellcome Collection.
While miscarriage was coming under the purview of male physicians, some American women were concurrently interpreting the event as a positive one. In January of 1874 Annie Van Ness, twenty-six years old and newly married, opened her diary entry by disclosing how “very cross and irritable” she was and remarking “I think I have a very good reason to feel ill humored.” The following month she reported “I don’t know that I am in much better humor than when I last wrote as the cause of it still exists.” Van Ness was pregnant and apparently not very pleased by the prospect, perhaps because her husband had lost a lot of money in the Panic of 1873 and the couple was severely economizing, including a relocation from New York City to Yonkers. Two weeks later, however, her mood improved: “Quite a change has come over the spirit of my dream since I last wrote, and I am happy again, a week ago last night I was taken sick at the supper table, I went to my room and retired early, to make a long story short I will say that the next day Ma told me she had seen her first grand child.” Van Ness quickly amended the report: “I just happened to think that any body might imagine from reading this that I had a baby, but I haven’t! It was only what they call a miss--,” (Van Ness, Diary).
In June of 1879, Mary Cheney wrote a letter to her husband Frank, while he was travelling for his successful silk production business, revealing her latest pregnancy: “I was not mistaken about myself when you went away. But it is all right. I am feeling perfectly well and everyone says I look so. I really believe this is getting to be my normal condition.” Cheney had spent the last 16 years in near-constant reproduction: pregnant with, birthing, and nursing nine children, (Cheney, letter of June 24, 1879).
The following month she updated her husband about her condition, this time telling him about the loss of this latest pregnancy. She opened the letter “O Bliss, O Rapture unforeseen! The imaginary number 10, whom I had already begun to love, is not a real entity as yet, and I hope will not be for a long time to come.” Unlike Annie Van Ness, who perhaps dreaded the cost of a pregnancy and child, Cheney was relieved to have a miscarriage because she already had nine children and her youngest was only nine months old (Cheney, letter of July 9, 1879).
These positive emotions may seem inappropriate for the late-nineteenth century. At a time when most white American women were besieged with messages that their duty and natural destiny was to have children, these women were openly writing about how happy they were to fail in that duty. To be sure, women also expressed disappointment and grief in the wake of a miscarriage. For example, Lucretia Everett, a diplomat’s wife who spent most of her marriage travelling around Europe and mingling with royalty, described her multiple miscarriages as “misfortunes” and “unhappy circumstances” in her letters back home. Miscarriage does not hold one meaning, but myriad meanings that can change from day to day and person to person. In the cases of Cheney and Van Ness, that context included heavy restrictions on their abilities to have any control over the size of their families.
Reproductive Control
The 1840s to the 1860s was something of a commercial golden age for contraception for many American women. The Industrial Revolution, while separating many of these women from their mothers or other networks of familiar women who could pass along helpful advice about encouraging or preventing pregnancy, also helped to spur an increase in the availability of contraception in unprecedented ways. The vulcanization of rubber, developed in 1844, led to condoms, diaphragms, and post-coital douching syringes becoming much more durable, comfortable, and affordable. Improvement in pill manufacturing increased the array of contraceptive and abortifacient pills, tonics, and syrups that flooded the market. While women living in urban centres had better access to these new products, the print revolution gave space for entrepreneurs to market directly to rural and frontier women through mail-order catalogues or print ads in newspapers and magazines. Fertility control was everywhere.
But most golden ages come to an end, and this one did by the 1870s. As Black Americans claimed new freedoms and as immigration exploded with the majority now coming from new parts of the world deemed by most white Americans as too foreign, lawmakers also became newly concerned about which families were having babies and which ones were not. Fertility rates had been falling steadily throughout the nineteenth century, with the most precipitous drop between 1850 and 1900, but the sharpest decrease was among white women. Black and immigrant families, while still getting smaller were not shrinking at the same rate as white families. According to many white men in political, medical, and social power, in order to sustain white supremacy, these trends needed to be reversed.
For the Congress of 1873, one of the answers to these concerns came from a New York anti-vice crusader named Anthony Comstock. The federal Comstock Act of 1873 banned the use of the U.S. Postal Service to mail any number of obscene materials, including contraceptive devices and information. Very quickly, most states passed what we now call “mini-Comstocks” that banned the manufacture, advertisement, sale, publication, and, in the most stringent laws, the use of contraceptive methods and devices.
Around the same time, a group of elite white physicians was touring the country speaking before state legislatures about the evils of abortion. With little support from other physicians and even from religious leaders, Horatio Storer, Joseph Tabor Johnson, and others convinced their political allies that abortion was a threat to the “national character.” If abortion remained legal (as it had been since the birth of the nation), they reasoned, America would be overrun by groups deemed less valuable. By 1880, every state had passed a ban on abortion.
Thus, when Annie Van Ness and Mary Cheney wrote of their relief at having miscarriages, it was not only their personal circumstances (economic stress or reproductive exhaustion) that led to that joy but also their ability to have any measure of control over their fertility. Contraception and abortion were illegal, leaving unsafe black-market fertility control devices and concoctions or unreliable homemade methods as their only avenue for preventing or terminating pregnancy. In addition, Van Ness and Cheney were living in a new world that repeatedly told them, through advertisements, federal policies, and popular discourse, that, as white women, their fertility was the most important, that their having babies was going to save the country from the downfall to which it was currently headed. The racialized reproductive narratives and realities of reproductive control limitations in the late nineteenth century shaped women’s emotional responses to and emotional relationships with miscarriage.
Miscarriage in nineteenth-century America was at once a family matter and a medical concern, a personal joy and a national tragedy. White physicians saw miscarriage as a way to draw in potential paying patients, but only after they had the chance to perfect intrusive practices on poor women, immigrants, and women of colour. All the while, women continued to interpret the loss of a pregnancy in very personal and myriad ways. For some, like Lucretia Everett who had at least three miscarriages and never sustained a pregnancy to live birth, miscarriage was an occasion of sorrow, disappointment, and loss. But for others, like Cheney and Van Ness, it was a relief amidst a highly restricted world of fertility control. In the nineteenth century, as is the case still today, miscarriage could be a benefit, loss, and even both at the same time.
Bibliography
Brayton, Charles E. List of Births Attended, November 1874. Rubenstein Library, Duke University, Durham, N.C.
Cheney, Mary Bushnell. Letter to Frank Cheney, June 24, 1879. Cheney family papers, box 1, Sophia Smith Collection, Smith College, Northampton, Mass.
Engelmann, George. “Pregnancy, Parturition, and Childbed among Primitive People.” American Journal of Obstetrics and Diseases of Women and Children 15 (1881): 602–618.
Everett, Lucretia Peabody. Letters to Sarah Everett Hale, August 9, 1820, and March 20, 1823. Hale Family Papers, Sophia Smith Collection, Smith College, Northampton, Mass.
Garrigues, Henry J. “The Treatment of Abortion.” Medical News 71 (1897): 589–592.
Martin, Henry, A. “Of Miscarriage, and Especially of the Use of Loomis’ Forceps in its Management.” Chicago Medical Journal and Examiner 38 (1879) 578–591.
Pearson, John C. “Retained Placentae in Abortion.” Medical and Surgical Reporter 19 (1868) 219.
Shivers, C. H. “Retained Placenta; Removal.” Medical and Surgical Reporter 60 (1889): 439–440.
Van Ness, Annie L. Youmans. Diary of Annie Van Ness, 1864 to 1881.Alexandria, VA: Alexander Street Press, 2004.
Further Reading
Cooper Owen, Deirdre. Medical Bondage: Race, Gender, and the Origins of American Gynecology, Athens: University of Georgia Press, 2017.
Doyle, Nora. Maternal Bodies: Redefining Motherhood in Early America Chapel Hill: University of North Carolina Press, 2018.
Freidenfelds, Lara. The Myth of the Perfect Pregnancy: A History of Miscarriage in America. New York: Oxford University Press, 2020.
Leavitt, Judith Walzer. Brought to Bed: Childbearing in America, 1750-1950. New York: Oxford University Press, 1986.
Tone, Andrea. Devices and Desires: A History of Contraceptives in America. New York: Macmillan, 2002.
Withycombe, Shannon. Lost: Miscarriage in Nineteenth-Century America. New Brunswick: Rutgers University Press, 2018.
Created 20 October 2022