
t Charles Kingsley’s funeral in 1875 Dean Stanley delivered a sermon in which he told the congregation: ‘Artisans and working men of London, you know how he desired, with a passionate desire, that you should have pure air, pure water, habitable dwellings, that you should be able to share the courtesies, the elevation of citizens, and of Englishmen’ (Kingsley: 1877, 216). In a lecture, ‘The Science of Health’, which he had delivered three years earlier at the Birmingham and Midland Institute of which he was the President, Kingsley had argued that industrialization, the demographic expansion which it stimulated, and the unsanitary living conditions which housed the new proletariat, had created the need for working people to enjoy the ‘courtesies’ and civic ‘elevations’ which a radically enhanced urban environment would offer them. But his religious commitments took his campaigning for radical improvements in social welfare beyond questions of poverty and disease and he addressed the threat to the evolution of the British ‘race’ from the degeneration which industrialization was causing (Kingsley:1880, 8).
Kingsley recognized that industrialization had also radically damaged the natural environment. In the November 1854 Nineteenth Century, he argued that it had reduced rural England to a ‘desert’ in which the country was ‘black’, the trees no longer ‘luxuriant’, the streams no longer ‘crystal-clear’, the vegetation destroyed, and the atmosphere polluted. But paradoxically industrialization had made urban England a heavily populated man-made ‘desert’ because of the demographic explosion that industrial growth had caused. In 1750 there were 17 towns with populations of approximately 10,000, but by 1800 there were more than 50. In 1800 approximately 20 per cent of the English and Welsh populations lived in towns of more than 5,000 rising to 50 per cent in 1851 and to 80 percent by 1911. In 1840 the authors of Report from the Select Committee on the Health of Towns recorded that ‘The increase in population in England and Wales, in 30 years, from 1801 to 1831, has been something more than 47 per cent; the actual increase in the number of inhabitants of five of our most important provincial towns has very nearly doubled that rate’. The authors of the report specified the following increases: Birmingham 73%, Leeds, 99%, Liverpool 100% Glasgow 108%, and Manchester, 109% (iii). Expressed in actual numbers, Manchester’s urban demographic expansion exemplifies the overall pattern – its population grew from 75,000 in 1801, to 182,00 in 1831, and to more than 300,000 in 1851 (Wohl, 4).
The result was the urban nightmare to which Kingsley responded. The wars against the French that ended in 1815 had weakened a population, and a series of cholera epidemics in 1831-32, 1848-49, 1853-54, and 1866 further weakened (see Banerjee, ‘Cholera’). Although Cholera became notorious because it ‘acquired a sharply epidemical quality in the early nineteenth century’ and thereby ‘dominated the lives and work of doctors practising in working-class districts’ (Flinn, 10), it was not the only or the deadliest contagion that permeated the poorest urban areas. Between 1840 and 1900 cholera killed 128,000 people, but in the same period pneumonia killed 243,486 and tuberculosis 406,788 (Halliday, 58).
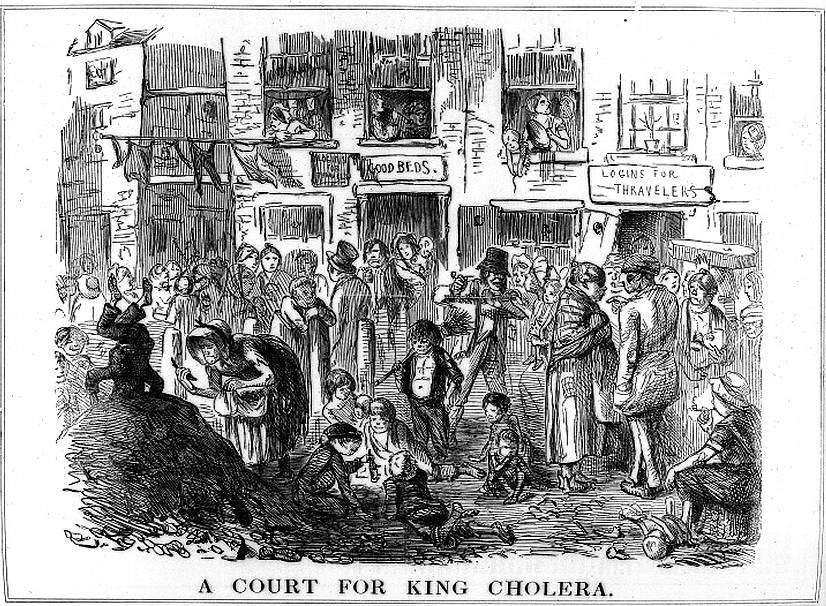
John Leech's cartoon in Punch, 23 (25 September 1852): 139), showing the association of cholera with squalor. A child stands on his head on top of a rubbish heap in the left-hand corner. An old woman scavenges from the heap, another child shows off his own find, and washing flutters in the breeze overhead. Credit: Wellcome Library, London. Many thanks to the Wellcome Library, London, which kindly allows images from its Digital Gallery to be used under this Creative Commons License for educational and non-commercial purposes. — — Jacqueline Banerjee [Click on the image to enlarge it.]
Overcrowded dwellings, unsanitary conditions and poverty were the major factors that spread the contagions among the new industrial proletariat. In Clinical Lectures on the Contagious Typhus epidemic in Glasgow and the Vicinity during the years 1831 and 1832 Richard Millar, Regius Professor of Materia Medica at Glasgow University from 1831 to 1833, recorded that in 1796, 7,000 of Liverpool’s inhabitants had lived in dank unventilated cellars and 9,000 in back-to-back houses. His comment on the result was terse: ‘fever was everywhere’ (10). The Nottingham Borough Records show that in 1840 8,000 of 11,000 proletarian dwellings were back-to-back, an arrangement which was particularly unhygienic (IX, 71), and Lord James Stuart of the Select Committee on the Health of Towns (1840) asked W. H. Duncan, a doctor from Liverpool: ‘You conceive that there are 124,000 of the working classes of Liverpool, living in either in those unhealthy cellars, or those neglected and miserable courts?’ Duncan replied: ‘Yes; but I should state that there are many front houses in the streets that are even worse than those in the courts; what are called lodging-houses, where there thirty or forty collected sometimes in one house’. The Commissioners also found that in Liverpool 86,000 people lived in 2,400 courts and 38,000 in cellars (p. 146, 2459-2460) and that in Manchester, the capital as it may be called of the cotton trade with a population of not less than 240,000 nearly 15,000 of the poorer inhabitants, 'constantly inhabit cellars' (x).
In his 1842 report Chadwick went out of his way to foreground these social conditions: ‘First, as to the extent and operation of the evils which are the subject of this inquiry: -That the various forms of epidemic, endemic, and other disease caused, or aggravated, or propagated chiefly amongst the labouring classes by atmospheric impurities produced by decomposing animal and vegetable substances, by damp and filth, and close and overcrowded dwellings prevail amongst the population in every part of the kingdom, whether dwelling in separate houses, in rural villages, in small towns, in the larger towns - as they have been found to prevail in the lowest districts of the metropolis’ (422). This was an incontestable statement in view of the evidence that supported it, and he reinforced the importance of social conditions by separating standards of material living from the frequency of epidemics: ‘high prosperity in respect to employment and wages, and various and abundant food, have afforded to the labouring classes no exemptions from attacks of epidemic disease, which have been as frequent and as fatal in periods of commercial and manufacturing prosperity as in any others’ (422).
Millar’s findings, however, contradicted this, for he was among those who were insisting on the closest connection between the spread of contagions and poverty. He argued in Clinical Lecturesthat typhus ‘often attacks the more indigent portion of our operatives, during those periodical suspensions of industry that, of late years, have caused so much distress among that part of our population’ (11); and his experience enabled him to articulate the connections between poverty and ‘fever’, i.e. typhus or ‘typhoid’:‘among the circumstances inducing typhus, by lowering the powers of life, none are found of more fatal, and irresistible efficacy, than the privations of extreme indigence, or poverty’, and he carefully listed the privations: poor diet, inadequate winter clothing, insufficient fuel for heating, depression, and ‘other enfeebling passions of the mind’ (6). Millar described typhus as ‘the poor man’s disease’ (12), and Robert Cowan, first Regius Professor of Medical Jurisprudence and Forensic Medicine at Glasgow University from 1839 to 1841, described typhus in the 1840 Journal of the Royal Statistical Society as ‘that unerring index of destitution’ (289).
In 1849 the Nottingham Borough Records provided further evidence that poverty favoured the spread of contagion. The Borough Sanitary Committee recorded that 'this terrible scourge the Cholera fixed itself in 1832 in Streets and Courts filthy, ill ventilated and crowded with inhabitants too poor, dirty or dissipated to procure necessary food or use the most common means to secure health' (my italics; IX, 71). On Sunday 7 January 1866, several years before Kingsley lectured on ‘The Science of Health’, Thomas Huxley took advantage of the bi-centenary of the bubonic plague of London to deliver his lay sermon at St. Martin’s Hall ‘On the Advisability of Improving Natural Knowledge’. He spelled out history’s lessons in what had become the standard account, stipulating the conditions that helped diseases proliferate: ‘unswept and ungarnished residences’; ‘narrow, un-watered streets, foul with accumulated garbage’; and ‘ill-drained, ill-lighted, ill-ventilated’ houses inhabited by ‘ill-washed, ill-clothed’ people. In such conditions, he said, echoing Millar and Cowan, ‘typhus is our companion, and cholera our visitor’ (342).
Men like Millar and Cowan contributed to the humanitarian medical work that reached its most important public form in Chadwick’s An Inquiry into the Sanitary Condition of the Labouring Population of Great Britain. But in the main conclusions to his Report Chadwick keeps his eye firmly on the public purse in a mixture of concern for social welfare and the exigencies of local and national budgeting. For instance, he argues persuasively that the cost to tenants and owners of public measures to ensure good drainage, cleansing, and a good water supply will be offset by the reduced cost of tending to the ill (221). He also reports that the Commissioners have no funds to pay for doctors who should be advised that they are to work gratis so that they can consider the financial loss which they might incur and whether they would be able to find means of compensating themselves for the loss (xiii).
Chadwick also offers financial inducements to persuade the authorities to take measures against unsanitary living conditions, inadequate heating and cleaning facilities, and the ‘stagnant pools or other outdoor nuisances’, and he argues that the most important measures are ‘drainage, the removal of all refuse of habitations, streets, and roads, and the improvement of the supplies of water’. He acknowledges that the cost of labour and cartage have militated against ‘the immediate removal of decomposing refuse of towns and habitations’. However, appealing to his audience’s thrift, he argues that ‘this expense may be reduced to one-twentieth or to one-thirtieth, or rendered inconsiderable, by using water and self-acting means of removal by improved and cheaper sewers and drains’. He quotes the case of a foreman of a brewery who is married to a ‘healthy wife’ (§ 77). She has given birth to seven children of whom six have died while still young ‘from diseases evidently springing from impure air’ — the culprit a badly built cesspool. Since the couple cannot afford to put things right, Chadwick suggests a neat balance between loss and gain: ‘the actual expenses of structural measures of prevention would not, as an entire outlay, have amounted to half the apothecary’s bill for drugs in the first case, a child sent to the country, who has come back refreshed, and has fallen ill again and died, or of the expenses of the funerals (superadded to the expenses of drugs) in the second case’, the other five children. The solution is to find a way to pay for the building improvements, and Chadwick proposes the following arrangement: ‘if the expenses of those structural arrangements were defrayed by an annual payment of instalments of principal and interest, spread over a period of 30 years, or a period coincident with the benefit, the expense of the extended or combined measure of prevention would not be more than £11. 15s. 10d. per tenement (£228 in modern values), or perhaps a small proportion of that sum, to the individual family’ (18). He does not concern himself with issues with which the foreman and his family would have been concerned, beginning with, ‘Who’s going to lend us the money, and what will the rate of interest be? What will we do while the structural work is going on?’
Chadwick also balances vested interests with what we know as recycling and environmental concern when he proposes that refuse be put to profitable use and ‘the pollution of natural streams’ be avoided. He also has the public purse in mind when he argues that investment in public drainage, supplies of water laid on in houses, and improved cleansing will reduce the existing charges incurred by sickness and premature deaths. But he does not lose sight of the main objective whereby the ‘means of diminishing atmospheric impurity’ will almost completely eradicate the ‘noxious agencies’.
Chadwick’s mindfulness of the public purse proved futile. Influential Parliamentarians opposed the proposed expenditure on the new proletariat whose labour created the wealth which many of them enjoyed. The minority Conservative administration headed by Robert Peel, the grandson of Robert ‘Parsley’ Peel, a wealthy cotton manufacturer, rejected the report. However, in February 1848, with another outbreak of cholera imminent, Lord Morpeth reintroduced a bill for promoting public health that passed into law as the 1848 Public Health Act whose provisions stimulated traditional British Tory opposition to imposing state control based on clear evidence. The Act did not require the Boards to appoint medical officers or compel them to undertake the cleansing programmes that Chadwick recommended. And the Act allowed the establishment of Local Public Health Boards only in areas where deaths from disease exceeded more than 23 per thousand, a figure that some bureaucrat had plucked Merlin-like from the sky. It was purely arbitrary and took no account of variations in age and local conditions.

Related material
- Sanitation and Disease in Rich and Poor
- G. M. Young on the creation of the Board of Health
- From Inconvenience to Pollution -- Redefining Sewage in The Victorian Age
- G. M. Young on the Factory Act of ’47, as the turning-point of the age
- The Drain Demon. — A Hard case
- Fun (a rival of Punchon Poverty and Starvation in England
Bibliography
Chadwick, E. Report on the Sanitary Condition of the Labouring Population of Great Britain: Supplementary Report on the Results of a Special Inquiry into the Practice of Interment in Towns. Made at the Request of Her Majesty’s Principal Secretary of State for the Home Department London: W. Clowes and Sons, 1843.
The Sanitary Condition of the Labouring Population of Great Britain. Ed. M.W. Flinn. Edinburgh: Edinburgh University Press, 1964.
Halliday, S. The Great Filth. London: Cassell & Company Ltd., 2007.
Journal of the Royal Statistical Society . [Coverage: 1838-1886]. 1.1 (49.4). London: Wiley for the Royal Statistical Society.
Kingsley, C. His Letters and Memories of His Life: ed. by his wife. London. Henry S. King & Co., 1877.
Kingsley, C. Sanitary and Social Lectures. London: Macmillan & Co., 1880.
Millar, R.Clinical Lectures: Contagious Typhus, Epidemic in Glasgow and the Vicinity during the years 1831 and 1832 Edinburgh: Adam Black, 1833.
Parliamentary Select Committee. Report from the Select Committee on the Health of Towns. London: J. M. Dent & Sons Ltd., 1914.
Records of The Borough of Nottingham , Vol. IX (1849). Manuscripts and Special Collections, University of Nottingham.
Wohl.Endangered Lives. London: J. M. Dent & Sons, 1983.
Last modified 26 May 2020